

Participant details
While 648 patients were initially assessed for eligibility, after excluding 109 who did not meet the inclusion criteria, 539 patients were assessed at T1. Subsequently, during T2, T3, T4, and T5 visits, 526, 517, 491, and 448 patients, respectively, were analyzed. Thereafter, as 21 patients were excluded from the analysis, 112 total samples were lost; thus, 427 patients were assessed (Fig. 1).
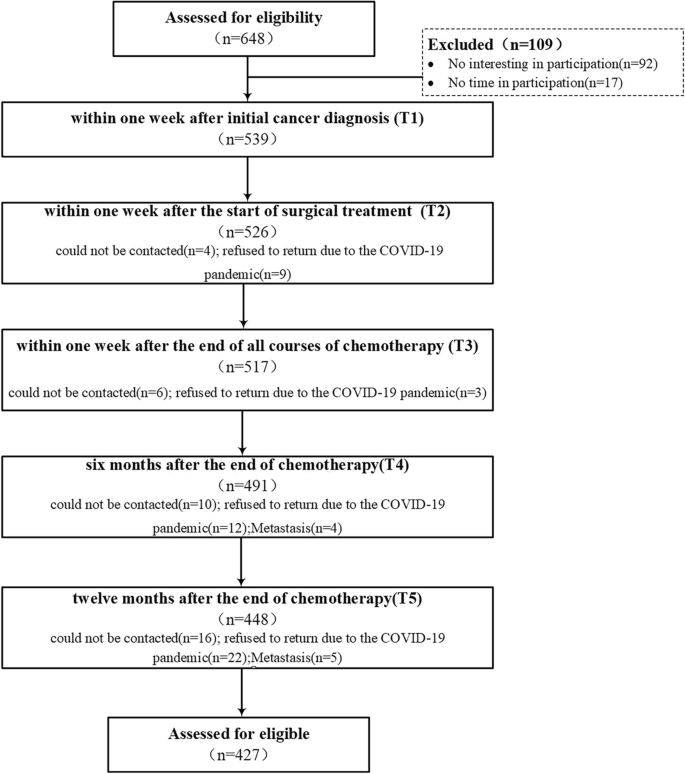
A difference test was performed between all data—both lost and valid—for the following variables: age (χ2 = 2.087, P = 0.554), education (χ2 = 1.258, P = 0.739), stage of tumor (χ2 = 1.640, P = 0.441), whether to keep the breasts (χ2 = 0.175, P = 0.675), employment (χ2 = 0.353, P = 0.838), having or not having minor children (χ2 = 0.457, P = 0.499), type of health coverage (χ2 = 0.472, P = 0.790), and monthly family income per capita (χ2 = 0.682, P = 0.711). There were no significant differences, indicating no structured loss among this study’s participants. The results are detailed in Table 1.
Description of variables and analysis of development trajectory
Figure 2 shows the average scores for SD, CRF, PD, and QoL at different measurement timepoints, during which each variable showed normal distributions at 0.734 (< 3) and 1.174 (< 10) for maximum absolute kurtosis and skewness, respectively27, thus facilitating subsequent analyses.
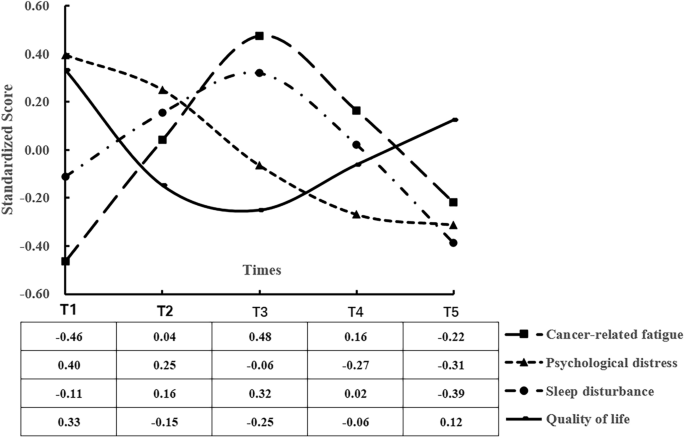
Variables’ development trajectory diagram.
Correlation analysis
Correlation analysis was used to explore the correlation between the four variables (Table 2). The five measurements of each variable all showed a certain stability. The correlation coefficient between measurements was in the range of 0.341–0.558 for CRF, 0.201–0.474 for PD, 0.301–0.564 for SD, and 0.152–0.478 for QoL.
3Latent growth model
Table 3 shows the fit indices of the linear and quadratic growth models. The nonlinear growth model has a statistically significant and better fit index than the linear growth model. Hence, there is a non-linear developmental relationship among CRF, PD, SD, and QoL. Table 4 shows the parameter estimation results of the nonlinear latent variable growth model.
The initial CRF level was statistically significant and greater than 0 (Intercept = 2.166, P < 0.001), and CRF showed an upward trend over the five surveys (slope = 0.649, P < 0.001), although the growth rate gradually weakened (quadratic = − 0.150, P < 0.001). The variance of the intercept, slope, and quadratic equation were all statistically significant and greater than 0, indicating statistically significant individual differences in the initial CRF level and its developmental speed and trend.
The initial PD level was significantly greater than 0 (intercept = 7.525, P < 0.001), and PD showed a significant weakening trend over the five surveys (slope = − 0.583, P < 0.001), although the weakening speed was gradually moderated (quadratic = 0.051, P < 0.01). The variances of the intercept, slope, and quadratic of PD were all significantly greater than 0 (P < 0.001), indicating statistically significant individual differences in the initial level, linear development trend, and rate of change.
The initial SD level was statistically significant and greater than 0 (Intercept = 0.580, P < 0.001), and SD showed an increasing trend (slope = 0.345, P < 0.001) during the five investigations, although the increase rate gradually dropped (P < 0.001, quadratic = − 0.099), indicating statistically significant differences in the initial level, linear development trend, and rate of change among individuals (P < 0.001).
The initial QoL level was statistically significant and greater than 0 (intercept = 2.393, P < 0.001), and the QoL showed a statistically significant weakening trend during the five surveys (slope = − 0.373, P < 0.001), although the weakening speed was gradually moderated (P < 0.001, quadratic = 0.087), indicating statistically significant differences in the initial level, linear development trend, and rate of change among individuals (P < 0.001).
Parallel growth model
To explore the influence of CRF, PD, and SD on QoL, the parallel impact model of the growth factors among variables was set based on the quadratic growth model (Fig. 3). The model fit indices (χ2 = 244.873, df = 120, RMSEA = 0.049, CFI = 0.948, TLI = 0.918, SRMR = 0.038) all met the criteria. The initial levels of CRF (coefficient = − 0.233, P < 0.01), PD (coefficient = − 0.296, P < 0.01), and SD (coefficient = − 0.388, P < 0.001) each had a statistically significant negative effect on the initial level of QoL. The linear development rate of PD was statistically significant, and negatively affected the linear development rate of the QoL (coefficient = − 0.305, P < 0.05), and the quadratic development rate of SD negatively affected the quadratic development rate of QoL (coefficient = − 0.391, P < 0.05). The remaining relationship paths were not statistically significant (P > 0.05).
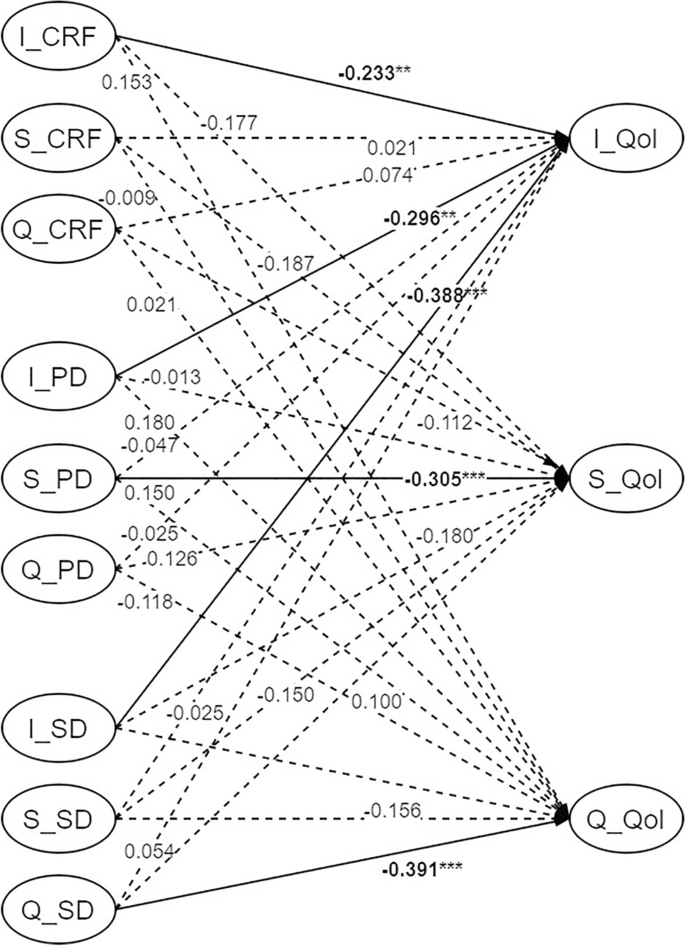
Parallel impact relationship model diagram. Note Significant paths are solid lines; Non-statistically significant paths are dashed; I = Intercept, S = Slope, Q = Quadratic, **P < 0.01; ***P < 0.001.
Cross-lagged panel models
The cross-model fitting indices (χ2 = 267.883, df = 120, RMSEA = 0.054, CFI = 0.935, TLI = 0.900, SRMR = 0.075) showed that all model fit indices meet the standard criteria, indicating that the model is supported by the data and has a good structure (see in Supplementary Table 1).
The autoregressive path results show that prior moment CRF, PD, SD, and QoL have a significant positive effect on the autoregressive path of the subsequent moment (P < 0.001), indicating that each variable at the prior moment significantly promotes development at the next moment.
Cross-lagged regression path analysis result (Fig. 4) show that PD within one week after diagnosis (T1) has a significant negative effect on QoL within one week after surgery (T2) (P < 0.05, β = − 0.127). CRF, PD, and SD within one week after surgery (T2) have a significant negative impact on QoL within one week after all chemotherapy sessions (T3) (P < 0.05), with standardized coefficients of − 0.109, − 0.137, and − 0.181 respectively. CRF, PD, and SD within one week after chemotherapy (T3) have a significant negative impact on QoL within six months after chemotherapy (T4) (P < 0.05), with standardized coefficients of − 0.101, − 0.137, and − 0.128 respectively. CRF, PD, and SD within six months after chemotherapy (T4) have a significant negative impact on QoL within twelve months after chemotherapy (T5) (P < 0.05), with standardized coefficients of − 0.130, − 0.113, and − 0.162 respectively.
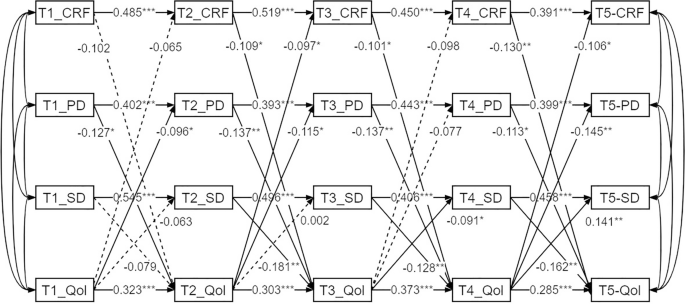
Cross-lag model path diagram. Note Significant paths are solid lines; Non-statistically significant paths are dashed; T1 = within one week after the initial cancer diagnosis, T2 = within one week after the start of surgical treatment, T3 = within one week after the end of all courses of chemotherapy, T4 = six months after the end of chemotherapy, T5 = 12 months after the end of chemotherapy; *P < 0.05; **P < 0.01; ***P < 0.001.
Additionally, QoL within one week after diagnosis (T1) has a significant negative effect on PD within one week after surgery (T2) (P < 0.05, β = − 0.096). QoL within one week after surgery (T2) has a significant negative effect on CRF and PD within one week after all chemotherapy sessions (T3) (P < 0.05), with standardized coefficients of − 0.097 and − 0.115 respectively. QoL within one week after chemotherapy (T3) has a significant negative effect on SD within six months after chemotherapy (T4) (P < 0.05, β = − 0.091). QoL within six months after chemotherapy (T4) has a significant negative effect on CRF, PD, and SD within twelve months after chemotherapy (T5) (P < 0.05), with standardized coefficients of − 0.106, − 0.145, and − 0.141 respectively. Other paths do not show significant effects between the various timepoints (P > 0.05).
link
:max_bytes(150000):strip_icc()/VWH-GettyImages-1488266051-624d29d61d3841d68b68daabf7f5f636.jpg "We Asked a Doctor What to Do If You’re Still Tired After 8 Hours of Sleep")






