

Setting and procedure
The Pregnancy and Birth Survey of the FHMS has been conducted every year since the March 11, 2011 disaster, targeting women who registered their pregnancies in Fukushima Prefecture during a specified time period each year. The pregnancy registration grants free access to antenatal care and well-child visits and is available to all pregnant women in Japan. Participants in the self-administered questionnaire survey were asked to respond by either mail or an online system that was available starting in FY201614.
Participants and recruitment
Survey in the postpartum period
In the FY2011 to FY2018 surveys, 115,976 cases satisfied either of the following conditions: receiving a Maternal and Child Health Handbook from a municipal office in Fukushima Prefecture, or receiving the handbook from an office outside of Fukushima Prefecture, but receiving antenatal care and giving birth in Fukushima Prefecture. In total, there were 58,350 responses, of which 57,958 were valid and 392 were invalid (blank, invalid responses, not qualified as respondents). Of the respondents, we analyzed 56,481 cases, excluding 729 that received Maternal and Child Health Handbooks outside of Fukushima Prefecture and 748 that did not involve live births. In Japan, there is a custom known as “sato-gaeri”, or returning to one’s parents’ home when the time for childbirth approaches and giving birth while receiving support from one’s mother. Therefore, we excluded those who received their Maternal and Child Health Handbook outside of Fukushima Prefecture and gave birth in Fukushima Prefecture because they were likely to have lived in Fukushima Prefecture for only a short period of time and were unlikely to have been affected by the radiation.
Follow-up survey at 4 years after childbirth
The target group consisted of 24,444 respondents of the FY2011-2014 Pregnancy and Birth Surveys who were identified as being alive along with their children by referring to municipal records (excluding those who miscarried, had their pregnancy terminated, or those who had a stillbirth). There were a total of 10,000 responses, of which all were valid. Of the respondents, we analyzed 9,860 cases, excluding 140 for which either the data on depressive tendency in the postpartum period or at 4 years after childbirth was missing (Fig. 1).

Participants in the pregnancy and birth surveys.
Data items
The main outcome indicator was depressive symptoms measured by a two-item screening tool to reduce the number of questions. This tool was developed by Wooley et al. for major depression. Mishina et al. evaluated its potential use as a brief screening tool to detect mothers with postpartum depressive symptoms15. This can be used to measure depressive symptoms 4 years after birth and correlates with the EPDS. In both the survey and survey 4 years later, we asked, “During the past month, have you often felt down, depressed, or hopeless?” and “During the past month, have you often found little interest or pleasure in doing things?” We classified women who answered “Yes” to one or both of these questions as positive for depressive symptoms. It has been reported that using the Edinburgh Postpartum Depression Questionnaire (EPDQ) as the standard, the sensitivity and specificity of the two-item screening tool was 88% and 76%, respectively15. Other associated factors were extracted from both surveys, and analyzed as follows.
Survey in the postpartum period
Maternal age was defined as of April 1 of the year following the survey. Regions that issued Maternal and Child Health Handbooks (registered regions) were classified into 6 areas: Kempoku, Kenchu, and Kennan comprise the central region, which is the most populated region. Kempoku had higher radiation levels than Kenchu, and Kennan. Soso and Iwaki comprise the coastal region. Soso is closest to the nuclear power plant and was a designated evacuation zone. Aizu is a mountainous region farthest from the nuclear power plant. Figure 2 shows the location of the six regions of Fukushima Prefecture and the average estimated external dose during the first 4 months by region. The average external dose during the first 4 months after the accident were estimated by Ishikawa et al.16.

Map of the Fukushima prefecture (Shown is the average estimated external dose during the first 4 months by region).
In response to the question on subjective health, “Do you think of yourself as healthy?”, respondents selected 1 of 4 answers ranging from “Very healthy” (1) to “Not healthy at all” (5). For the question, “Did you receive sufficient antenatal or delivery care for the current pregnancy?”, responses ranged from “Very much” (1) to “Not at all” (5). We categorized cohabiting family members into nuclear families and extended families. In response to the question, “Are you evacuated from your home?”, respondents selected 1 of the following 3 answers: “Under evacuation,” “Returned from evacuation,” and “Never evacuated.” Maternal confidence was assessed by the question, “Are there any moments when you do not feel confident about childrearing?”, to which responses of “Yes” or “Unsure” were classified as lacking maternal confidence, and “No” was classified as having maternal confidence. Intention to become pregnant again was assessed by the question, “Are you planning to become pregnant in the future?” The reasons for not intending to become pregnant again included the following: “Do not have a desire for it”, “Age or health-related reason”, “Busy raising children”, “Financial reason”, “Have no one to support me in housework/child rearing”, “Have no daycare service”, “Family living apart”, “Worried about the effects of radiation”, “Life as an evacuee”, and “Other”. This study used “Worried about the effects of radiation” in the analysis. In addition to not planning another pregnancy due to radiation concerns, we included avoiding breastfeeding due to “Concern about radiation contamination of breast milk” and free responses about “Effects of radiation on their child” as a radiation concern.
Follow-up survey at 4 years after childbirth
We assessed anxiety about radiation effects by the proportion of women who checked at least one box in response to the statement, “Check boxes for all matters of unease regarding the effects of radiation.” The possible responses included, “Water,” “Food,” “Child’s outdoor play,” “Child’s health,” “Prejudice,” “Genetic effects,” and “Other.” We also assessed these women’s feelings of anxiety about their child by the proportion who checked at least one box in response to the statement, “Check boxes for all matters of concern regarding your child.” The possible responses included, “Physical and mental development,” “Diseases,” “Lifestyle,” and “Other.” Items on subjective health, maternal confidence, and hospitalization of children were used, in addition to the two-item depression screening that assessed anxiety about radiation effects and anxiety about their child16.
Statistical analysis
We used data from the after-childbirth survey from FY2011 to FY2018 and applied the Mantel-Haenszel test to observe trends in the proportion of women who had “depressive symptoms” as well as those who commented in the free responses about “Effects of radiation on their child.” Next, we gathered data from 9,860 cases that responded to both the survey in the postpartum period (postpartum questionnaire) and the survey at 4 years after birth (follow-up questionnaire), and divided the cases into four groups as shown in Fig. 3: persistent depression (depressed at both survey points), developed depression (not depressed initially but developed depression at 4 years after childbirth), improved from depressive symptoms (depressed initially but had improved at 4 years after childbirth), and no depressed (not depressed at either point).
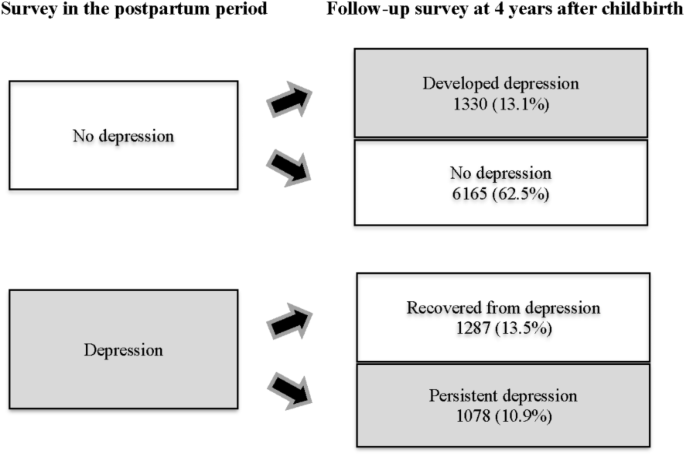
Analysis design: changes in postpartum depression (9,860 women in Fukushima Prefecture).
We compared the “developed depression” group with the “no depression” group and assessed the postpartum factors that were associated with maternal depressive symptoms at 4 years after childbirth. First, we used the chi-squared test to carry out univariate analysis of the following factors: disaster-related factors (registered regions, evacuation status, not intending to become pregnant again because of radiation effects, bottle-feeding because of radiation concerns, comments about effects of radiation on their child), maternal factors (age, parity, subjective health rating, family structure, medical history, maternal confidence), obstetric factors (received sufficient perinatal care, type of pregnancy, illness during pregnancy, delivery method), and child-related factors (sex of child, low birth weight, congenital anomaly). Then, we used multiple logistic regression analysis to investigate associations between developing depression at 4 years after childbirth and postpartum factors after adjusting for significant factors in the univariate analysis. Similarly, we compared the “improved from depressive symptoms” group with the “persistent depressive symptoms” group and determined which postpartum factors led to an improvement of maternal depressive symptoms at 4 years after childbirth. A p-value less than 0.05 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics 26.0.
Ethical considerations
This study was approved by the local ethics review committee of the authors’ institution (Approval No. 2021 − 223). The study was conducted in accordance with the Declaration of Helsinki, and all methods were performed in accordance with the relevant guidelines and regulations. The aims of the survey were detailed in a cover letter that was attached to the questionnaires sent to all the participants. By responding to the survey, written informed consent was obtained from all participants.
link





