

Data
We created an individual-level multi-year pooled cross-section using Medicaid administrative claims (Medicaid Analytic eXtract [MAX], January 2008-December 2012) from 16 Southern states (Alabama, Arkansas, Delaware, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, West Virginia) and the District of Columbia (DC) to identify enrollees with HIV9 and their demographic characteristics (e.g., age, race and ethnicity, sex), enrollment characteristics (e.g., payment type), and receipt of 5 annually recommended routine preventive care services: lipid screening, glucose screening, influenza vaccination, syphilis screening, and cervical cancer screening. We also used data on county-level HIV prevalence (AIDSVu, 2015), healthcare accessibility, socioeconomic status (Area Health Resources Files, 2010), and urbanicity (National Center for Health Statistics, 2013).
The primary data source, the MAX, is an ideal data source for this analysis. Medicaid is the largest insurance provider for PWH in the US, covering over 44% of adult PWH15. The MAX data used in this study represent a large, geographically diverse sample that includes both rural and urban individuals with HIV and those receiving care from both HIV-experienced and non-HIV experienced providers9. Further, the MAX data used in the current study approximate the current population of Medicaid enrollees with HIV, as the demographic composition, basis of eligibility (income, disability), percentage of enrollees from states that have not undergone Medicaid expansion (≈ 70% of enrollees in the current sample), and other quality of care measures are similar16,17. Finally, similarities between HIV specialist guidelines contemporaneous with the data (2009) and the most recent guidelines (2024) also support use of the data to describe patterns in service receipt for informing clinical practice today18,19.
Study sample
The sample population included adult Medicaid enrollees (aged 19–64 years) with HIV, identified using International Classification of Diseases, Ninth Revision (ICD-9) HIV diagnosis codes and verified using HIV-related Current Procedural Terminology (CPT) codes (e.g., quantification of HIV viral RNA) or National Drug Codes (NDC) for ART, as previously described9. Medicaid is the biggest US program supporting medical care and health services for low-income individuals20. Federal law requires that states cover specific groups, though flexibility regarding coverage for other populations is allowed20. Medicaid’s key eligibility groups include children, adults with disabilities, aged adults, and nondisabled adults20. Most individuals with HIV qualify through the disability pathway (41%)16. At the enrollee-level, we excluded enrollees ≥ 65 years and those dually eligible for Medicare or with evidence of private insurance to limit the sample to individuals for which the MAX data represented a complete record of clinical care. At the enrollee-year level, we excluded years with < 12 months of continuous enrollment per calendar year or with any missing individual or county-level characteristics in an enrollee-year. For the lipid, glucose, and cervical cancer screenings, enrollee-years with evidence of a lipid-related cardiovascular condition, diabetes diagnosis or, for women only, cervical cancer diagnosis (or previous abnormal cervical cancer screen) were excluded, respectively, as individuals with each condition (or diagnosis) would be ineligible for the screening (Fig. 1).
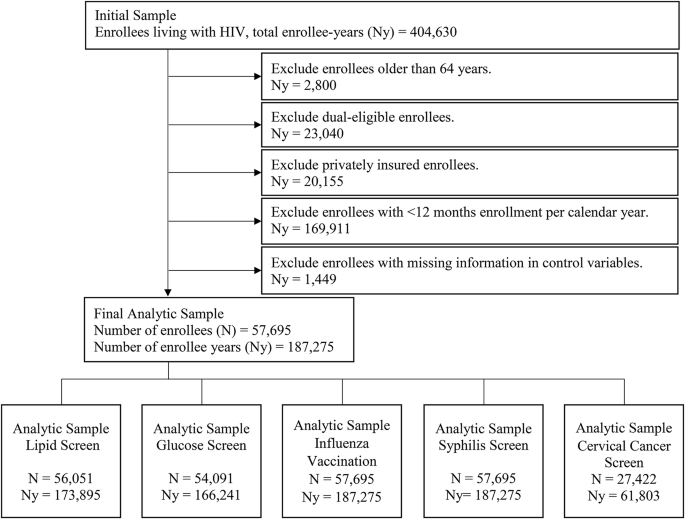
Flowchart for deriving the final analytic sample by outcome.
Outcomes
We examined five annual routine preventive care services: lipid screen, glucose screen, influenza vaccination, syphilis screen, and cervical cancer screen (women only) that were recommended by the HIVMA of the IDSA5. The recommendations specify (1) fasting lipid profile every 6–12 months, (2) fasting glucose every 6–12 months, (3) annual inactivated influenza vaccination, (4) annual syphilis screening for sexually active individuals (more often for those with risk-specific behaviors), and (5) annual pap smear in all women following two normal pap smears the first year of HIV diagnosis5. Receipt of a service was identified using CPT or NDC codes and defined as at least one screening or service in a given calendar year (January 1–December 31; see “Appendix”). The routine preventive services examined are important for several reasons. HIV infection increases the risk of certain lipid abnormalities, thereby increasing cardiovascular risk, and of diabetes, which may be due to the chronic inflammatory state associated with HIV infection and/or disruptions in lipid and glucose metabolism associated with certain antiretroviral medications21,22. Further, PWH are at higher risk of acquiring syphilis, and HIV/syphilis coinfection poses a greater risk of transmitting HIV due to the increased HIV viral load23,24. Finally, individuals with HIV are also at higher risk of influenza-associated morbidity and mortality, and women with HIV are four times more likely than HIV-negative women to be diagnosed with cervical cancer25,26.
Predictors
We included individual- and county-level variables that could impact receipt of quality HIV care. Control variables for individual-level demographics were race and ethnicity (Hispanic, Non-Hispanic Black, Non-Hispanic White, Non-Hispanic Other, Missing/Unknown), age at last observation (19–24, 25–34, 45–54, and 55–64 years), and gender (male, female). Presence of one or more coinfections (hepatitis B and/or C), of one or more comorbidities using non-AIDS-defining conditions27, and of an AIDS-defining condition28, controlled for individual health status (see “Appendix”). We controlled for urbanicity, designating enrollees residing in metropolitan statistical areas with ≥ 50,000 population as urban and those residing in nonmetropolitan areas with < 50,000 population as rural29. Finally, we controlled for participation in the Medicaid managed care health delivery model, defined as ≥6 months per year enrollment in managed care, as this model may increase use of preventive care services30.
County-level characteristics controlled for community-level factors that impact quality of care. Variables included: percent of the population with less than a high school education, percent unemployed, and median household income. HIV prevalence and health care supply (e.g., number of primary care physicians) controlled for healthcare accessibility.
Statistical analysis
We used an individual-level, pooled cross-section of all enrollee-years to examine receipt of RPC services. Sample medians (continuous variables) and percentages (categorical variables) described the full sample. Generalized estimating equations were used to examine receipt of annual routine preventive services and account for within-enrollee correlation of outcomes across multiple enrollee-years31. The quasi-information criterion identified an independent correlation matrix as the best-fit correlation structure for the model. Logit link and binomial distribution were used to model the relationship and estimate the probability of annual receipt of each service, holding predictors constant at their mean (for individual-level demographic variables) and median (for county-level variables) values. All models included state and year fixed effects to control for unobserved time-invariant heterogeneity in healthcare systems and delivery across states. Two-sided tests were used with a threshold of p < 0.05 to assess statistical significance. Analyses were conducted in SAS version 9.4 (SAS Inc., Cary NC).
We examined different subgroups to understand receipt of routine preventive care services across specific populations. Subgroups included individuals requiring closer HIV management (Intensive Specialty Management), defined as presence of 1 or more AIDS-defining conditions, presence of HIV-related nephropathy, or pregnancy within a given enrollee-year. We also examined those requiring closer general health management (Intensive General Management), defined as the presence of one or more comorbidities (e.g., chronic heart failure, any malignancy) within a given enrollee-year32. We also examined individuals < 45 years (Younger Age), given that the increasing occurrence of certain conditions with age (i.e., cardiovascular conditions, diabetes) may result in higher guideline concordant screening among older populations and lower screening for younger populations33. We assessed enrollees in Medicaid managed care (Managed Care) to examine receipt of services specific to this healthcare delivery model30. Finally, given disparities in other quality measures of HIV care13 and a higher risk of certain conditions for Non-Hispanic Black PWH12,13, we examined the annual probability of receiving RPC services separately for Non-Hispanic Black and Non-Hispanic White enrollees.
Ethics approval
This study was approved by the Virginia Commonwealth University Institutional Review Board (IRB). Due to the nature of the data, the IRB granted a waiver of informed consent, and a waiver of authorization for access to protected health information, for all participants. All procedures were performed in accordance with relevant guidelines and regulations.
link





